
Un guide pour les personnes atteintes du SII persistant : comment la fonction du nerf vague est liée à la régulation de l’intestin et du cerveau, et ce que la recherche montre au sujet des dispositifs non invasifs étudiés pour le soutenir.
Concernant l'auteur. Star Freudenberg est le fondateur de la Star Freud Wellness Clinic dans le centre de Londres, créée en 2017. Les présentations intestinales fonctionnelles sont la plus grande catégorie dans sa pratique : SII, ballonnements persistants, symptômes digestifs post-infectieux et une vue d’ensemble des symptômes intestinaux qui ne se résolvent pas uniquement par un changement alimentaire. Elle a travaillé avec des milliers de clients dans cette catégorie au cours des huit dernières années, travaillant également aux côtés du NHS et parlant et enseignant largement sur la santé intestinale et le bien-être préventif. Au cours des dernières années, son intérêt clinique s’est étendu à l’axe intestin-cerveau et à la stimulation non invasive du nerf vague en tant qu’adjuvant émergent dans certains cas. Ce guide reflète son examen de la recherche actuelle ainsi que ce qu’elle voit dans la pratique clinique.

Dysfonctionnement de l’intestin et du système nerveux
Dans ce guide
- Pourquoi le modèle standard d’IBS est souvent insuffisant
- Symptômes du SII et dysfonctionnement intestinal persistant
- Auto-évaluation : le système nerveux fait-il partie de votre image intestinale ?
- La régulation du nerf vague et de l’intestin
- Comment la dysfonction vagale peut contribuer au SCIs
- Ce que la recherche montre
- Appareils SNV : comment ils fonctionnent et à quoi s’attendre
- Mécanisme d’action et calendrier prévu
- Considérations de sécurité
Lorsque je suis tombé sur le procès de Kovacic en Lancet Gastroenterol Hepatol – une étude randomisée, contrôlée contre placebo, rapportant qu’environ 59 % des adolescents souffrant de douleurs abdominales fonctionnelles ont obtenu une réduction cliniquement significative de la douleur après une stimulation du nerf auriculaire, contre 26 % dans le bras factice – j’ai commencé à examiner plus sérieusement la littérature gut-brain plus large.
Ce que j’ai découvert à la clinique, c’est qu’un groupe de clients reconnaissables était déjà arrivé au même endroit depuis l’autre direction : des années de progrès partiel grâce à des interventions axées sur l’alimentation et le microbiome, tout en sentant qu’une partie importante du problème n’était toujours pas résolue.
On estime que le syndrome du côlon irritable touche entre 10 et 15 % de la population mondiale, ce qui en fait l’une des maladies chroniques les plus courantes et les plus mal comprises dans le monde.
Pour beaucoup de gens, l’image des symptômes qu’ils décrivent dans la salle de consultation est cohérente : ballonnements abdominaux qui se développent tout au long de la journée, crampes qui ne suivent pas clairement un aliment spécifique, alternance de motifs intestinaux en une seule semaine, urgence qui a remodelé leur routine quotidienne, et un inconfort après les repas qui ne répond plus au protocole qu’ils suivent actuellement.
Malgré l’ampleur du SII, de nombreuses personnes qui en sont atteintes décrivent au mieux des années de progrès partiel : des symptômes qui s’installent temporairement avec une approche et reviennent avec une autre, des restrictions alimentaires qui s’étendent sans soulagement durable.
Pour certaines personnes, c’est parce que le modèle standard de gestion du SII, largement axé sur l’intestin lui-même, peut ne pas rendre pleinement compte d’un élément pertinent du tableau.
Des recherches récentes en neurosciences ont mis en évidence le rôle du système nerveux autonome, et du nerf vague en particulier, dans la régulation de la fonction intestinale à un niveau que les approches axées sur l’alimentation et le microbiome ne peuvent atteindre directement.
Pour un sous-ensemble de personnes atteintes du SII, une réduction du tonus vagal et une dérégulation de l’axe intestin-cerveau peuvent contribuer de manière significative à la persistance des symptômes, quelle que soit la prudence avec laquelle ils gèrent leur alimentation.
Ce guide examine ce que la recherche montre au sujet de la relation entre la fonction du nerf vague et le SCI, et évalue les dispositifs non invasifs qui ont été développés pour soutenir la régulation vagale dans un format pratique et accessible.
Symptômes du SII et dysfonctionnement intestinal persistant
Le SII et les troubles digestifs fonctionnels sont caractérisés par des symptômes gastro-intestinaux persistants en l’absence d’anomalie structurelle identifiable. Contrairement aux conditions avec des résultats pathologiques clairs, le SII existe à l’intersection de la physiologie intestinale et de la régulation du système nerveux, ce qui est une des raisons pour lesquelles les approches standard fournissent si souvent un soulagement incomplet ou incohérent.
Les manifestations courantes incluent :
Symptômes digestifs :
- Ballonnements et distension abdominales, qui s’accumulent souvent tout au long de la journée et sont plus prononcés le soir
- Crampes et douleurs abdominales dont le début, l’intensité et la localisation sont imprévisibles
- Habitudes intestinales modifiées : diarrhée, constipation ou une combinaison fluctuante des deux au cours de la même semaine
- Une urgence qui perturbe le travail, les déplacements et la planification quotidienne
- Gaz excessif, éructation ou sensation de pression piégée qui ne se résout pas avec une restriction alimentaire
- Nausée, satiété précoce ou sentiment persistant que la nourriture « fait fausse route », quel que soit ce qui a été mangé
- Réactions alimentaires incohérentes, le même repas produisant une réponse significative un jour et aucune le lendemain
Symptômes intestinaux-cérébraux :
- Une vigilance accrue autour des repas, de manger en compagnie et d’être loin de chez soi
- Pensées anxieuses anticipatoires avant de manger qui peuvent être difficiles à distinguer des symptômes physiques eux-mêmes
- Troubles de l’humeur, manque d’énergie et irritabilité qui suivent de près les poussées de symptômes
- Un sentiment persistant que l’intestin et le système nerveux s’influencent mutuellement dans un cycle que ni le régime alimentaire ni la médication n’ont complètement interrompu
Symptômes autonomes :
- Difficulté à s’installer ou à se détendre, même pendant le repos
- Sommeil perturbé, y compris difficulté à s’endormir, réveils fréquents ou sommeil non réparateur pendant les périodes de symptômes intenses
- Fatigue disproportionnée par rapport au niveau d’activité et qui ne se résout pas avec un repos adéquat
- Une tension ou une vigilance persistante en arrière-plan qui est difficile à expliquer
Symptômes systémiques :
- Fatigue persistante et manque d’énergie sans lien avec la qualité du sommeil ou l’effort
- Difficulté à se concentrer, en particulier pendant ou après les épisodes symptomatiques
- Sensibilité accrue au stress, avec une période de récupération physiologique prolongée
- Une image symptomatique qui s’étend au-delà de l’intestin : la fatigue, l’humeur, la cognition et le sommeil sont tous affectés en même temps que la digestion
L’impact fonctionnel d’un SCI est souvent sous-estimé.
Beaucoup de gens décrivent la construction de leur routine quotidienne autour des symptômes intestinaux (planifier les itinéraires, limiter les engagements sociaux, restreindre davantage leur alimentation au fil des années) et porter une charge cognitive qui est, avec le temps, aussi lourde que les symptômes eux-mêmes.
Symptômes intestinaux dus à une atteinte du nerf vague : auto-évaluation
The following is not a diagnostic tool, but it may help you identify whether the nervous system side of digestive regulation could be relevant to your experience.
Évaluez les symptômes que vous ressentez avec régularité :
Fonction digestive
- Ballonnements abdominaux qui s’accumulent tout au long de la journée, peu importe ce qui a été mangé
- Crampes ou douleurs qui ne sont pas systématiquement liées à un aliment ou à un repas spécifique
- Alternance de selles plus molles et de constipation dans la même semaine ou le même jour
- Une urgence qui nécessite une planification autour de l’accès aux toilettes
- Réactions digestives qui semblent inconstantes : la même nourriture provoque des symptômes imprévisibles
Réactivité du cerveau intestinal
- Des symptômes qui s’aggravent clairement et systématiquement pendant les périodes de stress, de mauvais sommeil ou d’anxiété accrue
- Des pensées anxieuses anticipées avant les repas, pas seulement un inconfort physique après eux
- Des symptômes intestinaux qui s’améliorent significativement pendant les périodes de calme ou de faible stress
- Événements émotionnels ou stressants déclenchant des épisodes digestifs, même sans changement alimentaire
- Le sentiment que l’intestin et le système nerveux réagissent au même signal sous-jacent
Signaux autonomes
- Difficulté à s’installer complètement, même pendant le repos
- Sommeil perturbé par une gêne intestinale, un état d’éveil ou une agitation sans cause claire
- Fatigue qui ne s’améliore pas proportionnellement au sommeil ou au repos
- Une réponse au stress qui prend plus de temps que prévu à se stabiliser après un événement ou une période difficile
Historique des symptômes
- Symptômes apparus ou s’étant considérablement aggravés après une infection gastro-intestinale, une période de stress extrême, une intervention chirurgicale ou une maladie grave
- Symptômes présents depuis plus de trois mois sans explication structurelle claire
- Une image symptomatique qui couvre plusieurs systèmes corporels : pas seulement la digestion, mais aussi l’énergie, l’humeur, la cognition et le sommeil
Capacité fonctionnelle
- Restriction alimentaire significative (suppression de plusieurs groupes alimentaires) avec seulement une amélioration partielle ou temporaire
- La routine quotidienne et les engagements sociaux modifiés pour s’adapter aux symptômes intestinaux
- Manger à l’extérieur, voyager ou être dans des environnements inconnus générant des pensées anxieuses significatives
- L’effort cumulatif de gestion des symptômes devenant aussi fatigant que les symptômes eux-mêmes
Historique des diagnostics et des traitements
- Enquêtes standard donnant des résultats normaux ou non explicatifs
- Un diagnostic formel de SII ou de trouble fonctionnel de l’intestin, ou une notification indiquant qu’aucune cause structurelle n’a été identifiée
- Plusieurs approches alimentaires, probiotiques et suppléments digestifs essayés sans résolution complète ou durable
- Prise en charge médicale standard fournissant un soulagement incomplet ou de courte durée
- Des investissements importants dans des stratégies de santé intestinale, accompagnés d’un sentiment persistant que quelque chose n’a pas encore été entièrement résolu
Si vous identifiez plusieurs caractéristiques dans les catégories de réactivité intestin-cerveau, de capacité autonome et fonctionnelle (en particulier si les symptômes persistent malgré l’intervention alimentaire et la prise en charge standard), la fonction du nerf vague et l’intestin-la régulation de l’axe cérébral peut être utile à considérer dans le cadre d’une vision plus large.
Chez certaines personnes, un tonus vagal réduit et un sevrage parasympathique peuvent contribuer à la gravité des symptômes d’une manière que les approches dirigées vers l’intestin seules ne peuvent pas traiter pleinement.
La stimulation du nerf vague peut valoir la peine d’être discutée avec votre professionnel de santé.
La connexion du nerf vague
Qu’est-ce que le nerf vague ?
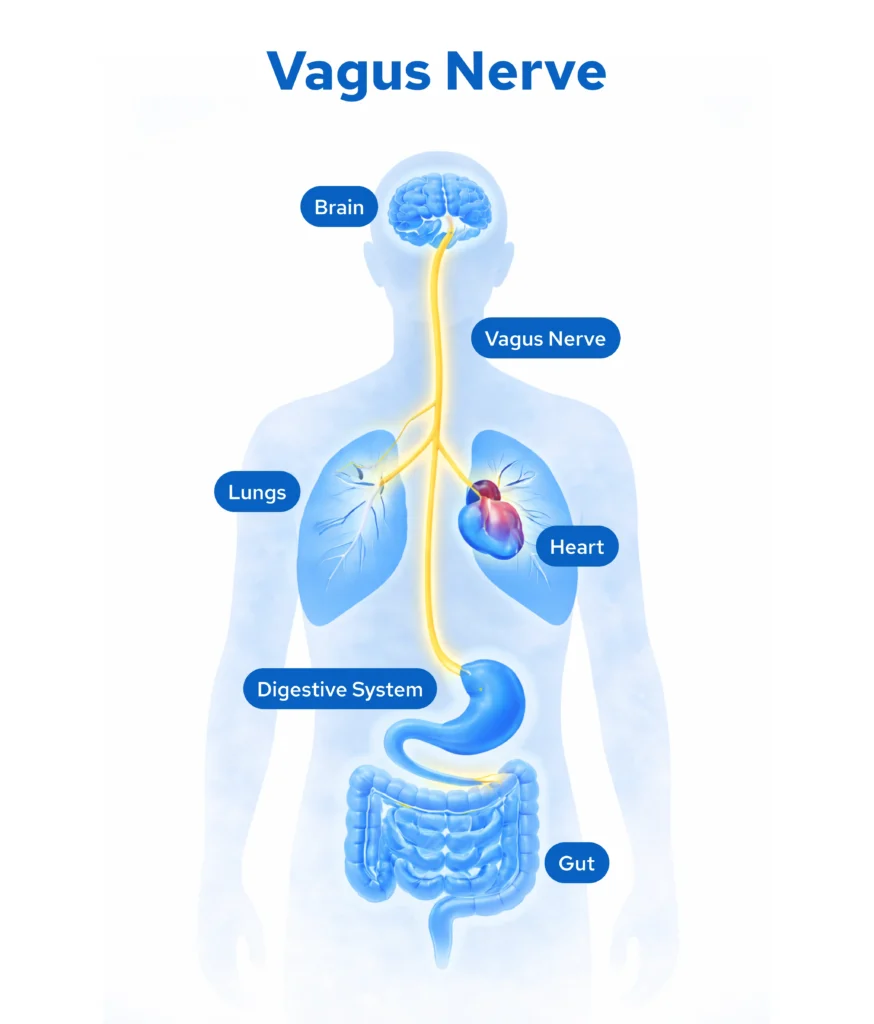
Le nerf vague (nerf crânien X) est le nerf le plus long et le plus complexe du système nerveux autonome, prenant naissance dans la moelle allongée et s’étendant à travers le cou, la poitrine et l’abdomen, où il communique directement avec le cœur, les poumons et le tractus gastro-intestinal.
Il est impliqué dans un large éventail de fonctions homéostatiques :
- Motilité gastro-intestinale, sécrétion et coordination des contractions musculaires digestives
- Traitement sensoriel viscéral et comment le cerveau reçoit et interprète les signaux de l’intestin
- Immune and inflammatory regulation via the cholinergic anti-inflammatory pathway
- Fonction de barrière intestinale et réponses immunitaires muqueuses localisées
- Régulation cardiovasculaire, y compris la fréquence cardiaque et la variabilité de la fréquence cardiaque
- Génération de modèle respiratoire
- Modulation de la réponse au stress et régulation émotionnelle grâce aux connexions avec les centres autonomes du tronc cérébral
Le système à deux modes
Votre système nerveux autonome fonctionne selon deux divisions complémentaires :
- Sympathique (écoulement thoracinaire) : Augmente le rythme cardiaque, élève la pression artérielle, mobilise l’énergie et supprime l’activité digestive non essentielle activée lors du stress, de la menace perçue ou de l’urgence.
- Parasympathique (écoulement vagal) : Contrôlé principalement par le nerf vague, il soutient la digestion, coordonne la motilité intestinale, facilite la restauration cellulaire et maintient l’état de repos et de digestion dans lequel la fonction digestive normale fonctionne.
Une fonction intestinale saine dépend de l’activité appropriée du système parasympathique pendant et après les repas sur le nerf vague, maintenant un tonus suffisant pour coordonner la motilité, réguler la sensibilité viscérale, gérer l’activité immunitaire localisée, et maintenir la communication intestin-cerveau qui maintient la digestion en arrière-plan sans devenir symptomatique.
Un stress prolongé, une maladie, une infection ou des périodes prolongées de dominance sympathique peuvent altérer le tonus vagal au fil du temps.
Lorsque cela se produit, l’intestin est laissé sans son régulateur principal et les ajustements alimentaires à eux seuls peuvent ne pas rétablir complètement cette régulation chez certaines personnes de l’intérieur même du tube digestif.
Comment le dysfonctionnement du nerf vague peut contribuer au SII et aux symptômes intestinaux persistants
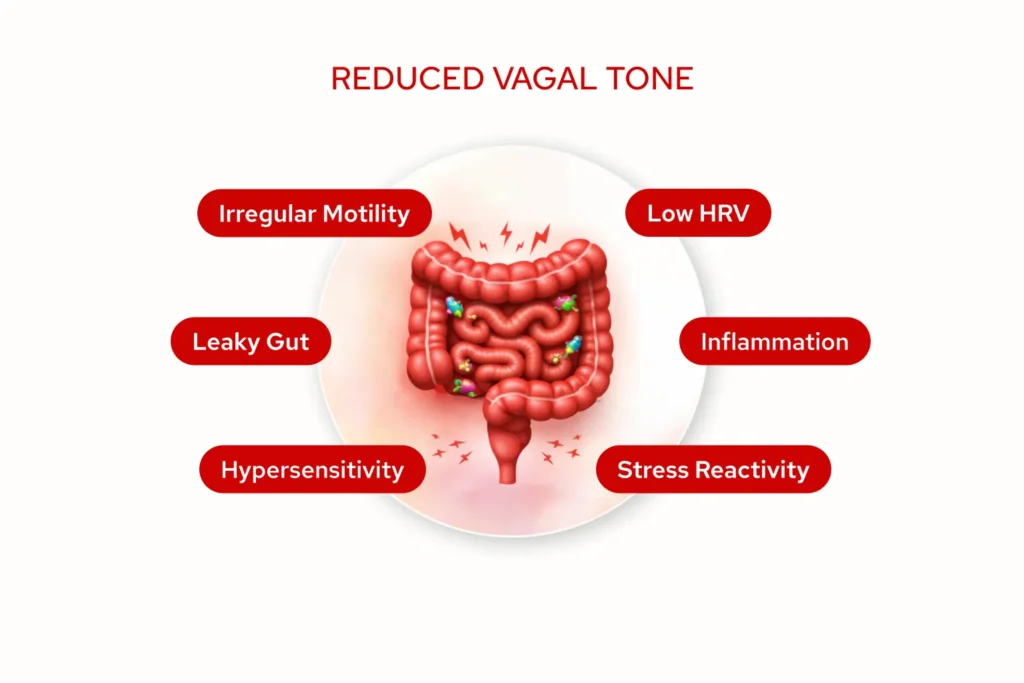
Lorsque le tonus vagal est réduit ou altéré, plusieurs éléments peuvent changer d’une manière directement liée à l’image des symptômes du SII :
- Dysrégulation de la motilité : Les contractions musculaires coordonnées qui déplacent les aliments dans le tractus digestif dépendent fortement de la signalisation vagale continue.
Lorsque le tonus vagal est réduit, la motilité peut devenir moins constante : trop rapide, trop lente ou variable selon les différentes parties de l’intestin.
Cela peut produire l’imprévisibilité qui caractérise l’expérience du SII chez de nombreuses personnes : urgence un jour, lenteur le lendemain, sans explication alimentaire claire qui s’applique à tout le cycle.
- Hypersensibilité viscérale : Environ 80 % des fibres du nerf vague transportent les informations sensorielles de l’intestin vers le cerveau.
Lorsque la régulation vagale est altérée, le seuil de perception des sensations digestives normales (gaz, distension intestinale, contractions musculaires ordinaires) comme inconfortables ou douloureuses peut chuter considérablement.
Cette sensibilisation centrale, dans laquelle le système nerveux interprète les signaux intestinaux comme plus menaçants qu’ils ne le seraient autrement, est maintenant reconnue comme un mécanisme central du SCI.
- Fonction de barrière intestinale altérée : L’activité vagale est impliquée dans le soutien de l’intégrité de la paroi intestinale et dans la régulation des réponses immunitaires localisées au sein de la paroi intestinale.
Lorsque le tonus vagal est réduit de manière chronique, une activation immunitaire de bas niveau et une perméabilité accrue de la barrière peuvent se développer, créant un environnement intestinal plus réactif et plus enclin à une hypersensibilité continue.
Ce mécanisme semble particulièrement pertinent dans le SII post-infectieux.
- Dysrégulation inflammatoire : Le nerf vague joue un rôle dans la voie anti-inflammatoire cholinergique, l’un des principaux mécanismes du corps pour moduler l’activité immunitaire et inflammatoire au sein du système gastro-intestinal.
Lorsque cette voie est sous-active, la signalisation inflammatoire de bas grade peut persister sans régulation appropriée, contribuant à une réactivité muqueuse qu’une restriction alimentaire ne résoudra probablement pas.
- Réduction de la variabilité du rythme cardiaque (HRV) : HRV est un marqueur validé et mesurable du tonus vagal.
Les personnes atteintes du SII présentent systématiquement une réduction significative de la VFC par rapport aux témoins sains, et le degré de cette réduction est corrélé à la gravité des symptômes et à l’altération de la qualité de vie.
Cela peut refléter le même retrait parasympathique qui perturbe également la régulation intestinale.
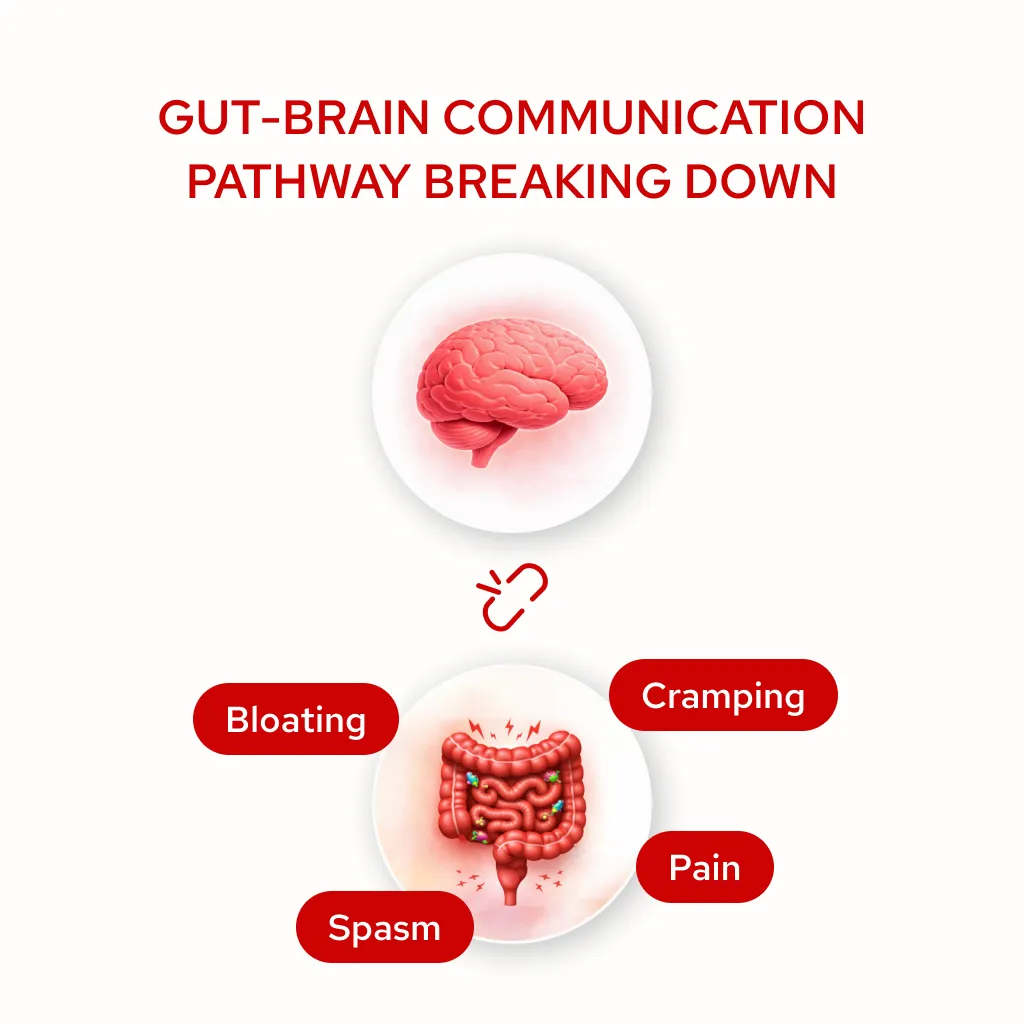
- La boucle de rétroaction stress-intestin : Lorsque le tonus vagal est bas, la dominance du système nerveux sympathique tend à devenir l’état par défaut. Cela maintient un fond de vigilance physiologique qui alimente directement la réactivité intestinale.
Les symptômes intestinaux génèrent des pensées anxieuses. Les pensées anxieuses amplifient l’hypersensibilité viscérale. L’augmentation de la sensibilité génère davantage de symptômes.
Au fil du temps, ce schéma peut devenir auto-renforçant de sorte que l’ajustement alimentaire ne puisse pas interrompre sa racine parce que la boucle est neurologique et non nutritionnelle.
Il est important de noter que le SII est une condition hétérogène plutôt qu’une entité pathologique unique. La dysfonction du nerf vague ne tient pas compte de tous les cas, et ce cadre ne sera pas pertinent pour tout le monde.
Certains individus ont principalement des schémas induits par le microbiome, d’autres une sensibilité alimentaire ou des caractéristiques post-infectieuses, et beaucoup présentent des mécanismes qui se chevauchent.
La dérégulation vagale semble plus pertinente chez les personnes ayant une VRC réduite, des schémas de symptômes corrélés au stress, l’apparition d’un SII post-infectieux ou des symptômes qui s’étendent au-delà de l’intestin pour inclure la fatigue, l’humeur, les troubles du sommeil et une réactivité systémique plus large.
Preuve scientifique
Des recherches publiées ont commencé à établir des relations plus claires entre la fonction du nerf vague et la physiopathologie du SII :
- Profil de dysfonctionnement autonome : Des études documentent systématiquement que les personnes atteintes du SII présentent des différences autonomes mesurables par rapport aux témoins sains, notamment une variabilité réduite de la fréquence cardiaque et une activité parasympathique altérée.
HRV (un marqueur validé du tonus vagal) est significativement plus faible dans les populations atteintes du SII, et le degré de réduction suit à la fois la gravité des symptômes et l’altération fonctionnelle. Cela suggère que, pour un sous-ensemble significatif de personnes atteintes du SII, la réduction du tonus vagal fait partie du tableau physiologique, et n’est pas simplement une conséquence secondaire du stress.
- Hypersensibilité viscérale et sensibilisation centrale : La recherche démontre que l’altération du traitement central des signaux intestinaux est un mécanisme central dans les troubles digestifs fonctionnels.
Le système nerveux reçoit des informations ordinaires de l’intestin, mais les interprète comme menaçantes ou douloureuses à des seuils significativement plus bas que chez les individus en bonne santé.
Cette sensibilisation centrale est physiologiquement cohérente avec une régulation vagale altérée de l’intestin.la boucle de rétroaction cérébrale et les études examinant la relation entre le tonus vagal et le seuil de douleur viscérale dans le syndrome du côlon irritable ont montré qu’une activité parasympathique réduite est indépendamment associée à des seuils de douleur plus faibles et à un fardeau symptomatique plus important.
- Recherche sur la stimulation du nerf vague et les symptômes intestinaux : Un nombre croissant de travaux examine les effets de la stimulation transcutanée du nerf vague sur la régulation intestin-cerveau et les symptômes digestifs. Des études sur le SCI et les populations atteintes de troubles fonctionnels de l’intestin ont rapporté :
- Améliorations des scores composites des symptômes gastro-intestinaux, notamment ballonnements, douleurs, impériosité et irrégularité intestinale, par rapport aux participants ayant reçu un traitement factice
- Améliorations mesurables de la VFC après des protocoles de stimulation soutenue, compatibles avec la restauration du tonus vagal comme mécanisme plausible
- Réductions de l’hypersensibilité viscérale et améliorations de la régularité intestinale
- Réduction des pensées anxieuses et de la fatigue qui accompagnent couramment les troubles digestifs persistants
- Un profil de sécurité généralement favorable dans l’ensemble de la recherche, sans événements indésirables graves rapportés dans les populations concernées par le SII
Cette recherche est encore en cours de développement, et elle n’est pas encore suffisante pour faire des affirmations définitives sur les résultats. Il fournit cependant une justification scientifique raisonnable pour considérer la neuromodulation vagale auriculaire comme une approche d’appoint chez des individus sélectionnés.
- SII post-infectieux : Le SCI post-infectieux (se développant à la suite d’une infection gastro-intestinale importante) est associé à des marqueurs de troubles vagaux, à une activité inflammatoire élevée et à une perméabilité accrue de la barrière intestinale.
Ces résultats sont cohérents avec la perturbation des voies régulatrices et anti-inflammatoires vagales par l’événement infectieux d’origine, créant une dérégulation autonome qui persiste bien au-delà de l’infection elle-même.
Cette population peut être particulièrement pertinente pour la neuromodulation vagale dans le cadre d’une stratégie de rétablissement plus large.
- L’image mécaniste : La recherche suggère que l’adressage de la régulation vagale peut influencer la coordination de la motilité, la sensibilité viscérale, la signalisation immunitaire et la fonction de barrière intestinale par le biais d’une voie partagée, ce qui aide à expliquer pourquoi les améliorations des symptômes observées dans certaines études couvrent ce qui semble être autrement des problèmes distincts.
Appareils VNS : comment ils fonctionnent et ce qu’il faut rechercher
De chirurgical à non invasif
Pendant de nombreuses années, la stimulation du nerf vague cliniquement établie n’était disponible que sous forme d’un dispositif implantable, une procédure chirurgicale nécessitant des réglages spécialisés, un coût important et un placement permanent.
Cela le rendait inaccessible pour la plupart des personnes qui gèrent des problèmes de santé chroniques en dehors de la neurologie ou de la psychiatrie spécialisées.
Plus récemment, la stimulation transcutanée du nerf vague (tVNS) est apparue comme une alternative non invasive. Ces dispositifs envoient des signaux électriques au nerf vague par la peau, sans chirurgie, implantation ou prescription.
Cela a créé de nouvelles possibilités d’explorer la neuromodulation vagale dans un format beaucoup plus accessible et pratique.
Ces appareils fonctionnent via deux points d’accès principaux :
- Cervical (cou) : Certains dispositifs ciblent la branche cervicale du nerf vague en plaçant des électrodes sur le côté du cou, près de l’artère carotide.

Le nerf vague coule superficiellement ici, et il peut être stimulé de manière transcutanée.
Cependant, cette approche implique la stimulation d’un faisceau nerveux mixte à un point où les fibres sympathiques, parasympathiques et autres sont très proches, ce qui rend l’engagement vagal précis et sélectif plus difficile à réaliser.
Les effets secondaires courants rapportés avec les dispositifs cervicaux (y compris la contraction des muscles du cou, le relâchement facial et l’élongation labiale) reflètent cette imprécision anatomique.
Pour une maladie comme le SII, où l’objectif est de soutenir spécifiquement la voie de régulation intestin-cerveau, c’est important.
- Auriculaire (oreille) : La branche auriculaire du nerf vague (ABVN) est une petite branche sensorielle qui alimente certaines parties de l’oreille externe, plus précisément le tragus et le cymba conchae.
Historiquement, la plupart des recherches sur la stimulation du nerf vague auriculaire se concentraient sur l’oreille gauche, en partie à cause de préoccupations théoriques précoces concernant les effets cardiaques associés à la stimulation vagale droite.
Cependant, des recherches plus récentes suggèrent que la stimulation contrôlée de la branche auriculaire droite peut également permettre un engagement vagal significatif, et le domaine continue d’évoluer à mesure que la compréhension de la neuromodulation autonome progresse.

C’est l’un des rares endroits où une branche d’un nerf crânien est accessible à la surface de la peau, ce qui le rend uniquement accessible pour une stimulation non invasive sans la complexité structurelle d’une approche cervicale.
Parce que la stimulation engage principalement les fibres vagales afférentes (les mêmes voies vagales afférentes impliquées dans la transmission des informations sensorielles entre l’intestin et le tronc cérébral), elle s’aligne plus directement avec la voie de régulation intestin-cerveau qui est pertinente dans le SCI. Cette spécificité anatomique est l’une des raisons pour lesquelles le point d’accès auriculaire a suscité beaucoup plus d’intérêt que les approches cervicales dans le contexte des troubles digestifs fonctionnels et de la régulation autonome.
La littérature clinique publiée sur les issues de santé gastro-intestinale, l’amélioration du HRV et l’hypersensibilité viscérale repose principalement sur des protocoles de stimulation auriculaire, pas cervicale.
Lorsque l’on considère un dispositif VNS spécifiquement pour le soutien de l’intestin et du cerveau, le point d’accès n’est pas simplement une préférence de conception. Il s’agit d’une variable significative permettant de déterminer si la stimulation est susceptible d’engager la voie concernée.
Mécanisme d'action
Lorsque l’on considère un dispositif VNS spécifiquement pour le soutien de l’intestin et du cerveau, le point d’accès n’est pas simplement une préférence de conception. Il s’agit d’une variable significative permettant de déterminer si la stimulation est susceptible d’engager la voie concernée.
- Modulation des neurotransmetteurs : La stimulation peut déclencher la libération d’acétylcholine au niveau des terminaisons parasympathiques, favorisant un passage de la dominance sympathique vers l’activité parasympathique et activant les voies anti-inflammatoires
- Activation du noyau du tronc cérébral : Les signaux vagaux afférents se projettent vers le noyau du tractus solitaire, qui intègre l’information régulatrice autonome et influence les centres de communication intestin-cerveau dans la moelle.
- Rééquilibrage autonome : Une stimulation constante peut favoriser un changement progressif de l’équilibre autonome, améliorant la HRV et réduisant potentiellement l’hypersensibilité viscérale au fil du temps.
- Adaptation neuroplastique : Les protocoles SNV soutenus peuvent soutenir la réorganisation des réseaux autonomes centraux, une considération importante étant donné que les changements sont progressifs plutôt qu’immédiats.
- Modulation inflammatoire : La stimulation vagale active la voie anti-inflammatoire cholinergique, ce qui pourrait aider à réduire la signalisation inflammatoire de bas grade associée au dysfonctionnement de la barrière intestinale et à la réactivité des muqueuses dans certaines présentations du SCI.
Paramètres scientifiques
Les protocoles de recherche pour la neuromodulation vagale utilisent généralement :
- Durée de la session : La plupart des protocoles recommandent une utilisation quotidienne de 30–60 minutes pour des résultats optimaux, bien que des séances plus courtes de 15 minutes puissent encore être bénéfiques pour certaines personnes.
- Difficulté : Calibré au seuil sensoriel individuel; perceptible mais confortable, sans douleur
- Cohérence, Application quotidienne pendant au moins 8–12 semaines, car les changements neuroplastiques et autonomes associés à cette approche nécessitent une utilisation soutenue et régulière.
Calendrier prévu
SNV soutient l’adaptation progressive du système nerveux plutôt que la suppression immédiate des symptômes. Selon les recherches disponibles :
Semaine 1–2 : Beaucoup de gens remarquent un léger changement dans leur réponse générale au stress pendant et après les séances, et certains signalent des améliorations modestes du sommeil. Les changements dans les symptômes digestifs sont généralement limités à ce stade.
Semaine 3–4 : Certaines personnes commencent à remarquer des changements dans la réactivité de l’intestin : les repas sont moins chargés, les épisodes de ballonnements et de crampes diminuent en intensité ou en fréquence, les motifs intestinaux deviennent légèrement plus constants.
Mois 2–3 : Pour les personnes qui répondent, des changements plus significatifs ont tendance à émerger au cours de cette période : une plus grande régularité intestinale, une sensibilité viscérale réduite, une amélioration de la HRV, un recours réduit aux stratégies de gestion des symptômes et une capacité croissante à tolérer des aliments précédemment évités.
Mois 3+ : Pour ceux qui continuent, une stabilisation accrue de la régulation intestin-cerveau, une réduction des pensées anxieuses et de la charge cognitive liées à l’intestin, ainsi qu’une amélioration de la capacité fonctionnelle, notamment une plus grande flexibilité en matière d’alimentation, de voyage et de planification.
Les réponses individuelles varient considérablement, et ces délais ne sont pas une garantie de résultats spécifiques. Cette approche est mieux utilisée comme une partie d’une stratégie plus large, considérée comme un soutien de l’intestin plutôt que comme une solution autonome.
Considérations de sécurité
La stimulation transcutanée du nerf vague auriculaire présente un profil de sécurité généralement favorable selon les recherches publiées. Les réponses transitoires potentielles peuvent inclure :
- Légère sensation de picotement au niveau du site de stimulation sur l’oreille
- En cas d’irritation temporaire localisée, certains protocoles peuvent alterner les oreilles pour réduire le contact répété au même site de stimulation, selon les recommandations du dispositif.
Attention : Cette approche n’est pas appropriée pour les personnes ayant un stimulateur cardiaque ou des dispositifs électriques implantés, pendant la grossesse ou chez celles qui ont des antécédents de vagotomie. Les circonstances individuelles comptent.
Si vous avez des antécédents médicaux complexes ou que vous prenez actuellement des médicaments affectant le système nerveux autonome, il est utile de consulter les directives relatives au dispositif et de parler avec votre professionnel de la santé avant de commencer.
Les symptômes intestinaux persistants liés à un dysfonctionnement du nerf vague et à une dérégulation de l’axe intestin-cerveau sont un domaine d’intérêt scientifique réel et croissant.
La recherche sur la neuromodulation vagale non invasive est encore en développement, mais elle est suffisamment substantielle pour faire de cette approche une approche raisonnable à explorer pour des individus sélectionnés, à côté plutôt qu’à la place d’autres stratégies.
Les informations contenues sur cette page sont fournies à des fins éducatives et ne constituent pas un avis médical spécifique ou se substituent à un diagnostic ou traitement professionnel. Les dispositifs de SNV ne sont pas destinés à diagnostiquer, traiter, guérir ou prévenir une maladie. Les personnes atteintes du SII ou présentant des symptômes intestinaux persistants doivent travailler avec des prestataires de soins de santé qualifiés afin d’élaborer des stratégies de prise en charge complètes et personnalisées. Consultez toujours votre médecin avant de commencer toute nouvelle intervention, en particulier si vous avez des antécédents médicaux complexes ou si vous prenez des médicaments. Recommandé par Star Freudenberg et la clinique de bien-être Star Freud en tant qu’approche d’appoint pour des patients sélectionnés chez qui une dysrégulation de l’axe intestin-cerveau semble constituer une partie cliniquement pertinente du tableau. Les résultats individuels peuvent varier.
Sources
- Bonaz B, Sinniger V, Pellissier S. Vagus nerve stimulation at the interface of brain-gut interactions. Cold Spring Harb Perspect Med. 2019;9(8):a034199.
- Bonaz B, Bazin T, Pellissier S. The vagus nerve at the interface of the microbiota-gut-brain axis. Front Neurosci. 2018;12:49.
- Farmer AD, Aziz Q. Visceral pain hypersensitivity in functional gastrointestinal disorders. Br Med Bull. 2009;91(1):123-136.
- Sowder E, Gevirtz R, Shapiro W, Ebert C. Restoration of vagal tone: a possible mechanism for functional abdominal pain. Appl Psychophysiol Biofeedback. 2010;35(3):199-206.
- Pellissier S, Dantzer C, Canini F, Mathieu N, Bonaz B. Psychological adjustment and autonomic disturbances in inflammatory bowel diseases and irritable bowel syndrome. Psychoneuroendocrinology. 2010;35(5):653-662.
- Mayer EA, Naliboff BD, Craig AD. Neuroimaging of the brain-gut axis: from basic understanding to treatment of functional GI disorders. Gastroenterology. 2006;131(6):1925-1942.
- Breit S, Kupferberg A, Rogler G, Hasler G. Vagus nerve as modulator of the brain-gut axis in psychiatric and inflammatory disorders. Front Psychiatry. 2018;9:44.
- Kovacic K, Hainsworth K, Sood M, et al. Neurostimulation for abdominal pain-related functional gastrointestinal disorders in adolescents: a randomised, double-blind, sham-controlled trial. Lancet Gastroenterol Hepatol. 2017;2(10):727-737.
Partager cet article :

