
En guide för personer med ihållande IBS: hur vagusnervfunktion relaterar till tarm-hjärnreglering, och vad forskningen visar om de icke-invasiva enheterna som studeras för att stödja den.
Om författaren. Star Freudenberg är grundaren av Star Freud Wellness Clinic i centrala London, grundat 2017. Funktionella tarmpresentationer är den största kategorin i hennes praxis: IBS, ihållande uppblåsthet, post-smittsamma matsmältningssymtom och den bredare bilden av tarmsymtom som inte löser sig genom dietförändring ensam. Hon har arbetat med tusentals klienter i denna kategori under de senaste åtta åren, också arbetat tillsammans med NHS och talat och undervisat i stor utsträckning om tarmhälsa och förebyggande wellness. Under de senaste åren har hennes kliniska intresse utvidgats till tarm-hjärnaxeln och till icke-invasiv vagusnervstimulering som ett framväxande tillägg i utvalda fall. Den här guiden återspeglar hennes granskning av den aktuella forskningen tillsammans med vad hon ser i klinisk praxis.

Gut and Nervous System Dysfunction
I den här guiden
- Varför standard IBS-modellen ofta kommer till kort
- Symtom på IBS och ihållande tarmdysfunktion
- Självbedömning: är nervsystemet en del av din tarmbild?
- Vagusnerven och tarmregleringen
- Hur vagal dysfunktion kan bidra till IBS
- Vad forskningen visar
- VNS-enheter: hur de fungerar och vad de ska leta efter
- Handlingsmekanism och förväntad tidslinje
- Säkerhetshänsyn
När jag stötte på Kovacic-rättegången i Lancet Gastroenterol Hepatol – en randomiserad, skamstyrd studie som rapporterade att cirka 59% av ungdomar med funktionell buksmärta uppnådde en kliniskt meningsfull minskning av smärta efter aurikulär nervstimulering, jämfört med 26% i skamarmen – Jag började titta på bredare tarm-hjärnlitteratur mer allvarligt.
Det jag hittade i kliniken var att en igenkännlig grupp klienter redan hade anlänt till samma plats från den andra riktningen: år med delvis framsteg genom kost- och mikrobiomfokuserade interventioner, samtidigt som jag kände att en viktig del av bilden förblev olöst.
Irriterande tarmsyndrom beräknas påverka mellan 10 och 15% av den globala befolkningen, vilket gör det till en av de vanligaste och mest ihållande missförstådda kroniska hälsotillståndet i världen.
För många människor är symptombilden som de beskriver i konsultationsrummet konsekvent: bukuppblåsning som bygger över dagen, kramper som inte spårar rent med någon specifik mat, alternerande tarmmönster inom en vecka, brådskande som har omformat deras dagliga rutin och obehag efter måltider som inte längre svarar på vilket protokoll de för närvarande kör.
Trots hur utbredd IBS är, beskriver många människor med det i bästa fall år av delvis framsteg: symtom som tillfälligt löser sig med en strategi och återvänder med en annan, kostbegränsningar som expanderar utan varaktig lättnad.
För vissa människor beror detta på att standardmodellen för IBS-hantering, till stor del fokuserad på själva tarmen, kanske inte helt står för en relevant bild.
Den senaste neurovetenskapliga forskningen har lyfts fram det autonoma nervsystemets roll, och vagusnerven i synnerhet, för att reglera tarmfunktionen på en nivå som kost- och mikrobiomfokuserade tillvägagångssätt inte direkt kan nå.
För en delmängd av personer med IBS kan minskad vagal ton och dysreglering i tarm-hjärnaxeln bidra meningsfullt till varför symtomen kvarstår, oavsett hur noggrant de hanterar mat.
Den här guiden tittar på vad forskningen visar om förhållandet mellan vagusnervfunktion och IBS och utvärderar de icke-invasiva enheterna som har utvecklats för att stödja vagal reglering i ett praktiskt, tillgängligt format.
Symtom på IBS och Persistent Gut Dysfunction
IBS och funktionella matsmältningsstörningar kännetecknas av ihållande gastrointestinala symtom i frånvaro av identifierbar strukturell abnormitet. Till skillnad från förhållanden med tydliga patologiska fynd finns IBS i skärningspunkten mellan tarmfysiologi och nervsystemreglering, vilket är en anledning till att standardmetoder så ofta ger ofullständig eller inkonsekvent lättnad.
Vanliga manifestationer inkluderar:
Matsmältningssymtom:
- Abdominal uppblåsthet och distension, ofta byggd över dagen och mest uttalad av kvällen
- Kramp- och buksmärta som är oförutsägbar vid början, intensitet och plats
- Förändrade tarmvanor: diarré, förstoppning eller en fluktuerande kombination av båda inom samma vecka
- Brådskande som stör arbete, resor och daglig planering
- Överdriven gas, bockning eller en känsla av fångat tryck som inte löser sig med kostbegränsning
- Illamående, tidig mättnad eller en bestående känsla av att mat "sitter fel" oavsett vad som har ätits
- Inkonsekventa matreaktioner, samma måltid ger ett betydande svar en dag och ingen nästa
Gut-hjärnsymtom:
- Ökad vaksamhet kring måltider, äta i sällskap och vara hemifrån
- Förväntande oroliga tankar innan du äter som kan vara svåra att skilja från de fysiska symtomen själva
- Humörstörningar, låg energi och irritabilitet som följer nära symptomfällningar
- En ihållande känsla av att tarmen och nervsystemet påverkar varandra i en cykel som varken kost eller medicinering helt har avbrutit
Autonomic symptoms:
- Svårigheter att sätta sig eller avveckla, även under vila
- Störd sömn, inklusive svårigheter att somna, ofta vakna eller uppfriskande sömn under högsymtomperioder
- Trötthet som är oproportionerligt med aktivitetsnivån och inte löser sig med tillräcklig vila
- En ihållande bakgrundsspänning eller vaksamhet som är svår att redogöra för
Systemiska symtom:
- Ihållande trötthet och låg energi som inte är relaterad till sömnkvalitet eller ansträngning
- Koncentrering av svårigheter, särskilt under eller efter symptomepisoder
- Ökad känslighet för stress, med en långvarig fysiologisk återhämtningsperiod
- En symptombild som sträcker sig bortom tarmen: trötthet, humör, kognition och sömn som alla påverkas tillsammans med matsmältningen
Den funktionella effekten av en IBS underskattas ofta.
Många beskriver att bygga sin dagliga rutin kring tarmsymtom (planeringsvägar, begränsa sociala åtaganden, begränsa sin diet ytterligare med varje år som går) och bära en kognitiv belastning som med tiden är lika betungande som själva symtomen.
Tarmsymtom På grund av Vagus Nerve Impairment Självutvärdering
Följande är inte ett diagnostiskt verktyg, men det kan hjälpa dig att identifiera om nervsystemets sida i matsmältningsregleringen kan vara relevant för din upplevelse.
Utvärdera symtomen du upplever med regelbundenhet:
Digestive Function
- Maguppblåsning som bygger över dagen oavsett vad som har ätits
- Kramp eller smärta som inte är konsekvent kopplad till en specifik mat eller måltid
- Växla mellan lösare avföring och förstoppning inom samma vecka eller dag
- Brådskande som kräver planering kring toalettåtkomst
- Matsmältningsreaktioner som känns inkonsekvent: samma mat orsakar symtom oförutsägbart
Gut-Brain Reactivity
- Symtom som är tydligt och konsekvent sämre under perioder med stress, dålig sömn eller ökade oroliga tankar
- Förväntande oroliga tankar före måltider, inte bara fysiskt obehag efter dem
- Tarmsymtom som förbättras meningsfullt under verkligt lugna eller låga stressperioder
- Känslomässiga eller stressande händelser som utlöser matsmältningsepisoder även utan dietförändring
- En känsla av att tarmen och nervsystemet svarar på samma underliggande signal
Autonoma Signaler
- Svårigheter att helt bosätta sig, även under vila
- Sömn störd av tarmbesvär, vakenhet eller rastlöshet utan klar orsak
- Trötthet som inte förbättras proportionellt med sömn eller vila
- Ett stressrespons som tar längre tid än väntat att lösa efter en svår händelse eller period
Symtomhistoria
- Symtom som började eller försämrades signifikant efter en gastrointestinal infektion, en period av extrem stress, operation eller en betydande sjukdom
- Symtom finns i mer än tre månader utan en tydlig strukturell förklaring
- En symptombild som sträcker sig över flera kroppssystem: inte bara matsmältning, utan energi, humör, kognition och sömn
Funktionell Kapacitet
- Betydande dietbegränsning (flera livsmedelsgrupper tas bort) med endast delvis eller tillfällig förbättring
- Dagliga rutinmässiga och sociala åtaganden ändrade för att tillgodose tarmsymtom
- Äta ute, resa eller vara i okända miljöer som skapar meningsfulla oroliga tankar
- Den kumulativa ansträngningen för symptomhantering blir lika trött som själva symtomen
Diagnostik och behandlingshistoria
- Standardundersökningar som returnerar normala eller icke-förklarande resultat
- En formell diagnos av IBS eller funktionell tarmstörning eller anmälan om att ingen strukturell orsak har identifierats
- Flera dietmetoder, probiotika och matsmältningstillskott försökte utan full eller varaktig upplösning
- Standard medicinsk hantering som ger ofullständig eller kortlivad lättnad
- Betydande investeringar i tarmhälsostrategier tillsammans med en bestående känsla av att något ännu inte har tagits upp helt
Om du identifierar dig med flera funktioner över tarm-hjärnreaktivitet, autonoma och funktionella kapacitetskategorier (särskilt om symtomen kvarstår trots dietinsats och standardhantering) kan vagusnervfunktion och regleringen av tarm-hjärnaxlar vara värt att betrakta som en del av den bredare bilden .
Hos vissa individer kan minskad vagal ton och parasympatisk tillbakadragande bidra till symptomens svårighetsgrad på sätt som tarmstyrda tillvägagångssätt ensam inte helt kan hantera.
Vagus nervstimulering kan vara värt att diskutera med din vårdgivare.
Vagus Nerve-anslutningen
Vad är Vagus nerv?
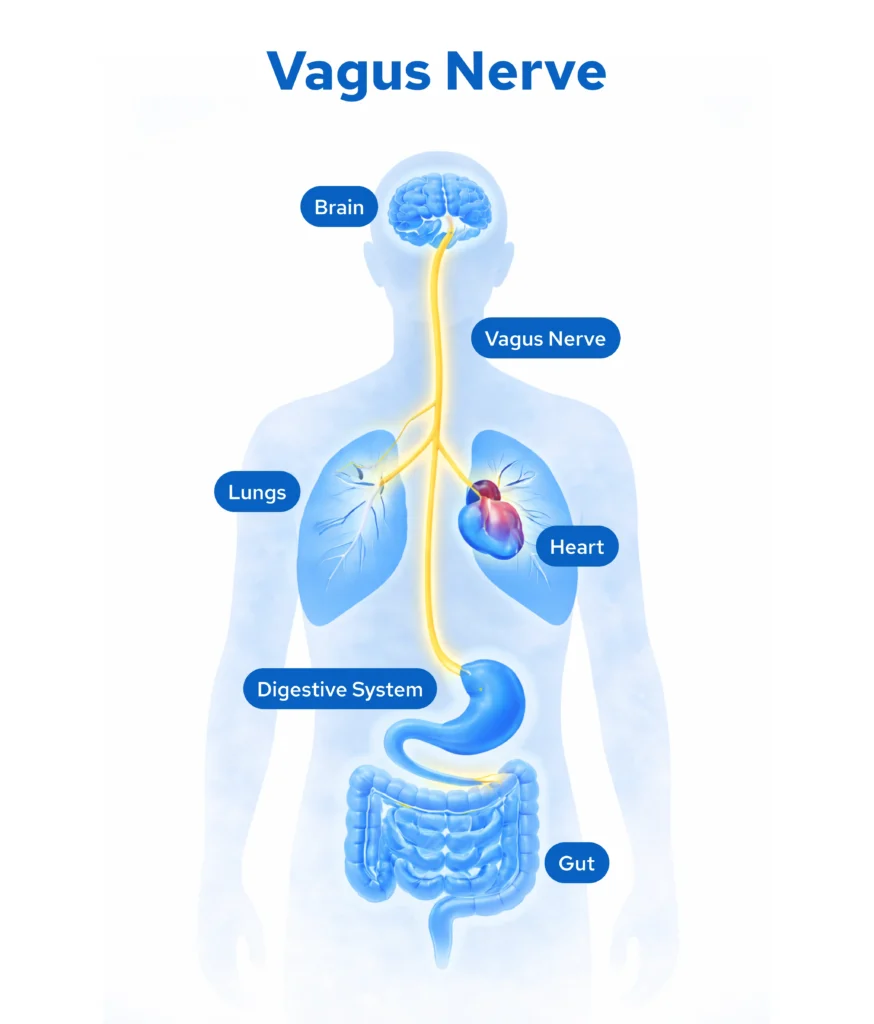
Vagusnerven (kranialnerven X) är den längsta och mest komplexa nerven i det autonoma nervsystemet, med ursprung i medulla oblongata och sträcker sig genom nacken, bröstet och in i buken, där det kommunicerar direkt med hjärtat, lungorna och mag-tarmkanalen.
Det är involverat i ett brett utbud av homeostatiska funktioner:
- Gastrointestinal rörlighet, utsöndring och koordination av muskelsammandragningar i matsmältningen
- Visceral sensorisk bearbetning och hur hjärnan tar emot och tolkar signaler från tarmen
- Immun- och inflammatorisk reglering via den kolinergiska antiinflammatoriska vägen
- Gutbarriärfunktion och lokala mukosala immunsvar
- Kardiovaskulär reglering, inklusive hjärtfrekvens och hjärtfrekvensvariabilitet
- Andningsmönstergenerering
- Stresssvarmodulering och emotionell reglering genom anslutningar till hjärnstammens autonoma centra
Två-lägesystemet
Ditt autonoma nervsystem fungerar genom två kompletterande divisioner:
- Sympatisk (thoracolumbar-utflöde): Ökar hjärtfrekvensen, höjer blodtrycket, mobiliserar energi och undertrycker icke-väsentlig matsmältningsaktivitet som aktiveras under stress, uppfattat hot eller brådskande.
- Parasympatisk (vagalt utflöde): Kontrolleras främst av vagusnerven, stöder matsmältningen, koordinerar tarmrörlighet, underlättar cellåterställning och upprätthåller det vila och smälta tillståndet där normal matsmältningsfunktion fungerar.
Hälsosam tarmfunktion beror på att det parasympatiska systemet är lämpligt aktivt under och efter måltiderna på vagusnerven och upprätthåller tillräcklig ton för att koordinera rörlighet, reglera visceral känslighet, hantera lokal immunaktivitet och upprätthålla mag-hjärnkommunikationen som håller matsmältningen igång i bakgrunden utan att bli symptomatisk.
Hållbar stress, sjukdom, infektion eller långvariga perioder med sympatisk dominans kan försämra vagal ton över tid.
När det händer lämnas tarmen utan dess primära regulator och enbart kostjusteringar kanske inte helt återställer den regleringen hos vissa individer inifrån själva tarmen.
Hur Vagus Nerve Dysfunction kan bidra till IBS och Persistent Gut Symptom
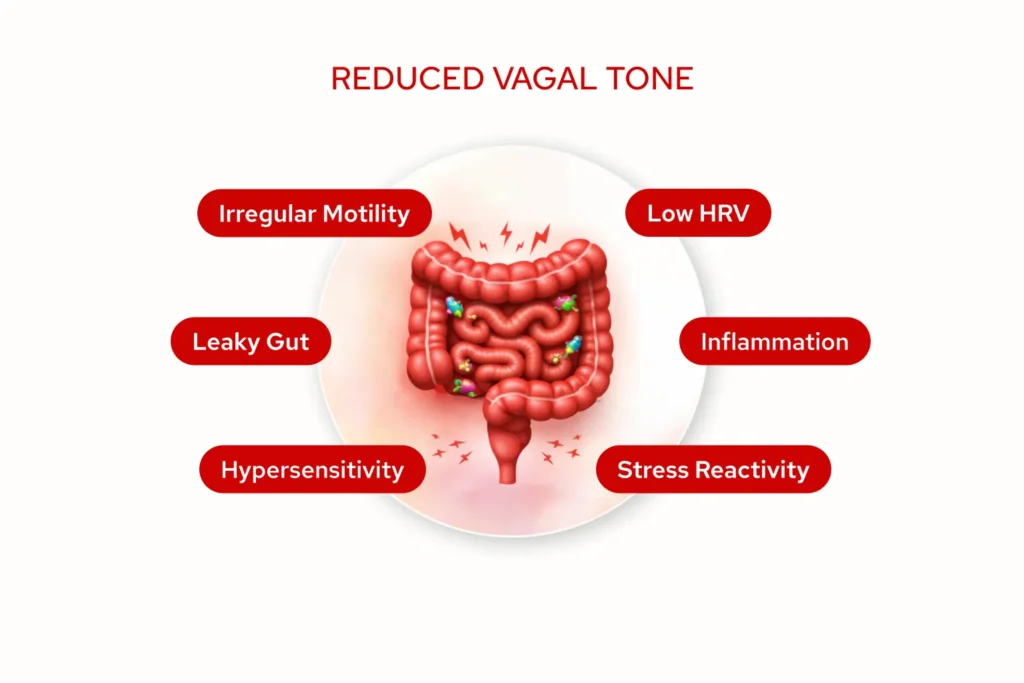
När vagal ton reduceras eller försämras kan flera saker förändras på sätt som är direkt relevanta för IBS symptombild:
- Motilitetsdyreglering: De samordnade muskelsammandragningarna som flyttar mat genom matsmältningskanalen beror starkt på kontinuerlig vagal signalering.
När vagal ton reduceras kan rörlighet bli mindre konsekvent: för snabbt, för långsamt eller varierande över olika delar av tarmen.
Detta kan ge den oförutsägbarhet som kännetecknar många människors upplevelse av IBS: brådskande en dag, tröghet nästa, utan tydlig dietförklaring som håller över mönstret.
- Visceral överkänslighet: Cirka 80% av vagusnervens fibrer har sensorisk information uppåt från tarmen till hjärnan.
När vagal reglering försämras kan tröskeln för att uppfatta normala matsmältningsupplevelser (gas, tarmspänning, vanliga muskelsammandragningar) som obekväma eller smärtsamma sjunka avsevärt.
Denna centrala sensibilisering, där nervsystemet tolkar tarmsignaler som mer hotande än de annars skulle vara, erkänns nu som en kärnmekanism i IBS.
- Nedsatt tarmbarriärfunktion: Vagal aktivitet är involverad i att stödja tarmfoderens integritet och att reglera lokala immunsvar i tarmväggen.
När vagal ton kroniskt reduceras kan lågkvalitativ immunaktivering och ökad barriärpermeabilitet utvecklas, vilket skapar en tarmmiljö som är mer reaktiv och mer benägen för pågående överkänslighet.
Denna mekanism verkar särskilt relevant i post-infektiös IBS.
- Inflammatorisk dysreglering: Vagusnerven spelar en roll i den kolinergiska antiinflammatoriska vägen, en av kroppens primära mekanismer för att modulera immun- och inflammatorisk aktivitet i mag-tarmsystemet.
När denna väg är underaktiv kan lågklassig inflammatorisk signalering kvarstå utan lämplig reglering, vilket bidrar till slemhinneaktiviteten som kostbegränsningen sannolikt inte kommer att lösa.
- Minskad hjärtfrekvensvariabilitet (HRV): HRV är en validerad, mätbar markör för vagal ton.
Personer med IBS visar konsekvent signifikant reducerad HRV jämfört med hälsosamma kontroller, och graden av denna minskning korrelerar med symptomens svårighetsgrad och livskvalitet.
Detta kan återspegla samma parasympatiska tillbakadragande som också stör störningen av tarmen.
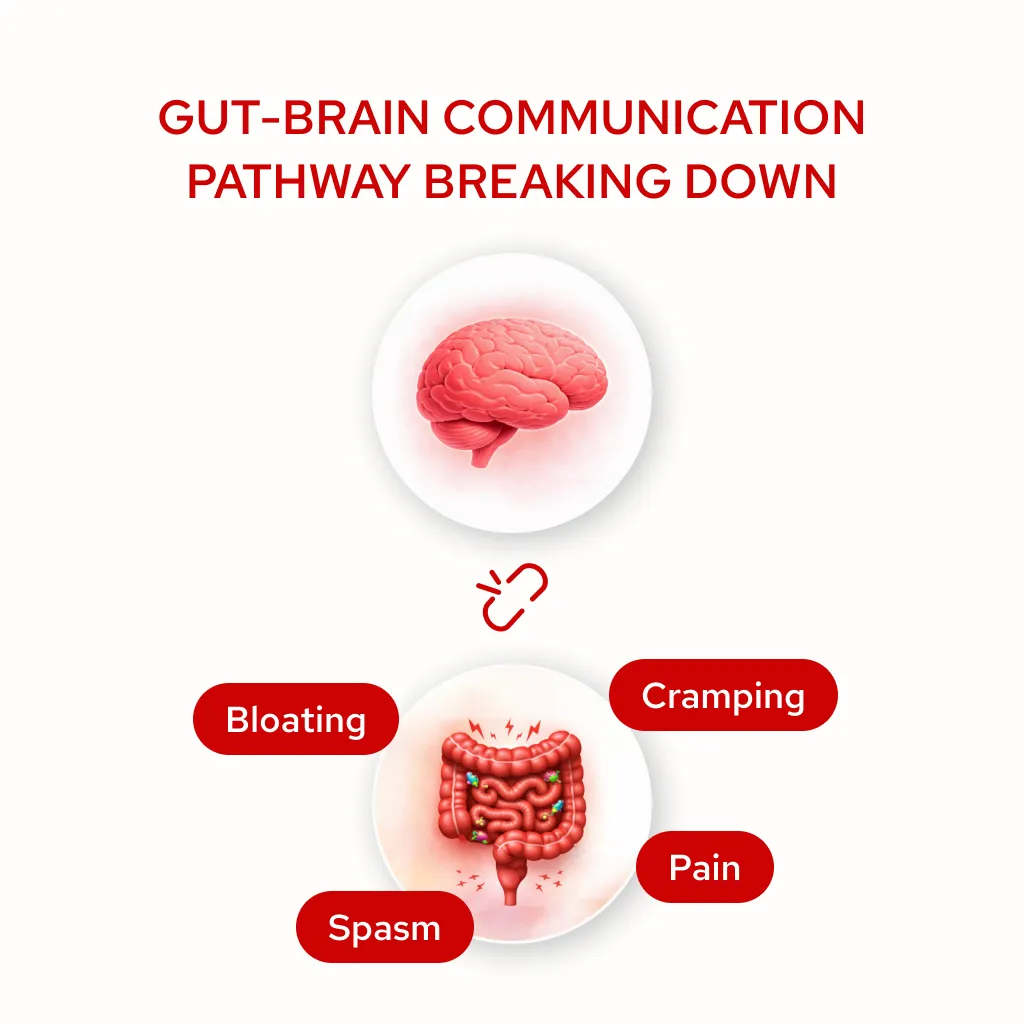
- Stress-tarmåterkopplingsslingan: När vagal ton är låg tenderar sympatisk nervsystemets dominans att bli standardtillståndet. Detta upprätthåller en bakgrund av fysiologisk vakenhet som matas direkt in i tarmreaktivitet.
Tarmsymtom genererar oroliga tankar. Ångestliga tankar förstärker visceral överkänslighet. Ökad känslighet genererar fler symtom.
Med tiden kan detta mönster bli självförstärkande på sätt som kostjustering inte kan avbryta vid dess rot eftersom slingan är neurologisk, inte näringsmässig.
Det är viktigt att notera att IBS är ett heterogent tillstånd snarare än en enda sjukdomsenhet. Vagus nervdysfunktion står inte för alla fall, och denna ram kommer inte att vara relevant för alla.
Vissa individer har främst mikrobiomdrivna mönster, andra kostkänslighet eller post-smittsamma funktioner, och många visar överlappande mekanismer.
Vagal dysreglering verkar mest relevant hos personer med reducerad HRV, stressrelaterade symptommönster, post-infektiös IBS-uppkomst eller symtom som sträcker sig bortom tarmen till att inkludera trötthet, humör, sömnstörningar och bredare systemisk reaktivitet.
Vetenskapliga bevis
Publicerad forskning har börjat etablera tydligare relationer mellan vagusnervfunktion och IBS-patofysiologi:
- Autonom dysfunktionsprofil: Studier dokumenterar konsekvent att individer med IBS visar mätbara autonoma skillnader från friska kontroller, inklusive minskad hjärtfrekvensvariabilitet och förändrad parasympatisk aktivitet.
HRV (en validerad markör för vagal ton) är signifikant lägre i IBS-populationer, och graden av reduktion spårar både symptomens svårighetsgrad och funktionsnedsättning. Detta antyder att för en meningsfull delmängd av personer med IBS är reducerad vagal ton en del av den fysiologiska bilden, inte bara en sekundär konsekvens av stress.
- Visceral överkänslighet och central sensibilisering: Forskning visar att förändrad central behandling av tarmsignaler är en kärnmekanism vid funktionella matsmältningsstörningar.
Nervsystemet får vanliga insatser från tarmen men tolkar det som hotande eller smärtsamt vid betydligt lägre trösklar än hos friska individer.
Denna centrala sensibilisering överensstämmer fysiologiskt med nedsatt vagal reglering av återkopplingsslingan i tarmen och hjärnan, och studier som undersöker förhållandet mellan vagal ton och visceral smärttröskel i IBS har funnit att minskad parasympatisk aktivitet är oberoende förknippad med lägre smärttrösklar och större symptombörda.
- Forskning om vagusnervstimulering och tarmsymtom: En växande mängd arbete undersöker effekterna av transkutan vagusnervstimulering på tarm-hjärnreglering och matsmältningssymtom. Studier i IBS och populationer av funktionell tarmstörning har rapporterat:
- Förbättringar av sammansatta GI-symptomresultat, inklusive uppblåsthet, smärta, brådskande och tarm oregelbundenhet, jämfört med skambehandlade deltagare
- Mätbara förbättringar i HRV efter långvariga stimuleringsprotokoll, i överensstämmelse med återställande av vagal ton som en rimlig mekanism
- Minskningar av visceral överkänslighet och förbättringar av tarmens regelbundenhet
- Minskningar i oroliga tankar och trötthet som vanligtvis åtföljer ihållande matsmältningsstörningar
- En generellt gynnsam säkerhetsprofil över hela forskningen, utan några allvarliga biverkningar rapporterade i IBS-relevanta populationer
Denna forskning utvecklas fortfarande och det räcker ännu inte att göra slutgiltiga resultatkrav. Det ger emellertid en rimlig vetenskaplig grund för att betrakta aurikulär vagal neuromodulering som ett komplement tillvägagångssätt hos utvalda individer.
- Post-infektiös IBS: Post-infektiös IBS (utvecklas efter en signifikant gastrointestinal infektion) är associerad med markörer för vagal nedsättning, förhöjd inflammatorisk aktivitet och ökad permeabilitet i tarmen.
Dessa fynd överensstämmer med störningar i vagala reglerande och antiinflammatoriska vägar genom den ursprungliga infektiösa händelsen, vilket skapar autonom dysreglering som kvarstår långt bortom själva infektionen.
Denna population kan vara särskilt relevant för vagal neuromodulering som en del av en bredare återhämtningsstrategi.
- Den mekanistiska bilden: Forskningen antyder att adressering av vagal reglering kan påverka rörlighetskoordination, visceral känslighet, immunsignalering och tarmbarriärfunktion genom en delad väg, vilket hjälper till att förklara varför symptomförbättringarna i vissa studier spänner över vad som annars verkar vara separata problem.
VNS-enheter: Hur de fungerar och vad de ska leta efter
Från kirurgisk till icke-invasiv
Under många år var kliniskt etablerad vagusnervstimulering endast tillgänglig som en implanterbar anordning, ett kirurgiskt ingrepp som krävde specialinställningar, betydande kostnader och permanent placering.
Detta gjorde det otillgängligt för de flesta som hanterade kroniska hälsotillstånd utanför specialistneurologi eller psykiatri.
På senare tid har transkutan vagusnervstimulering (tVNS) framkommit som ett icke-invasivt alternativ. Dessa enheter levererar elektriska signaler till vagusnerven genom huden: utan operation, implantation eller recept.
Detta har skapat nya möjligheter för att utforska vagal neuromodulering i ett mycket mer tillgängligt, praktiskt format.
Dessa enheter fungerar genom två primära åtkomstpunkter:
- Cervikal (hals): Vissa anordningar riktar sig mot vagusnervens livmoderhalsgren genom att placera elektroder på sidan av nacken, nära halsartären.

Vagusnerven rinner ytligt här, och den kan stimuleras transkutant.
Emellertid innebär detta tillvägagångssätt att stimulera ett blandat nervpaket vid en punkt där sympatiska, parasympatiska och andra fibrer springer i närheten, vilket gör exakt, selektivt vagalt engagemang svårare att uppnå.
Vanliga biverkningar rapporterade med livmoderhalsanordningar (inklusive nackmuskelkontraktion, ansiktsdropp och läppdrag) återspeglar denna anatomiska imprecision.
För ett tillstånd som IBS, där målet är att stödja den reglerande vägen för tarmen, är detta viktigt.
- Aurikulär (örat): Den aurikulära grenen av vagusnerven (ABVN) är en liten sensorisk gren som tillhandahåller delar av det yttre örat, särskilt tragus och cymba conchae.
Historiskt sett fokuserade de flesta aurikulära vagusnervstimuleringsforskningar på det vänstra örat, delvis på grund av tidiga teoretiska oro beträffande hjärteffekter förknippade med högersidig vagal stimulering.
Nyare forskning tyder emellertid på att kontrollerad stimulering av rätt aurikulär gren också kan uppnå meningsfullt vagalt engagemang, och fältet fortsätter att utvecklas när förståelsen för autonom neuromodulering fortskrider.

Det är en av de få platserna där en gren av en kranial nerv är tillgänglig på hudytan, vilket gör den unikt tillgänglig för icke-invasiv stimulering utan strukturell komplexitet i en livmoderhalsmetod.
Eftersom stimulering här främst engagerar afferenta vagala fibrer (samma afferenta vagala vägar som är involverade i överföring av sensorisk information mellan tarmen och hjärnstammen) överensstämmer den mer direkt med den reglerande vägen för tarmen som är relevant i IBS. Denna anatomiska specificitet är en anledning till att den aurikulära åtkomstpunkten har väckt betydligt mer forskningsintresse än cervikala tillvägagångssätt i samband med funktionella matsmältningsstörningar och autonom reglering.
Den publicerade kliniska litteraturen om tarmhjärnutfall, HRV-förbättring och visceral överkänslighet bygger främst på aurikulära stimuleringsprotokoll; inte cervikala.
När man överväger en VNS-enhet specifikt för tarm-hjärnstöd är åtkomstpunkten inte bara en designpreferens. Det är en meningsfull variabel i huruvida stimuleringen sannolikt kommer att gå in i den relevanta vägen.
Handlingsmekanism
När en kalibrerad elektrisk signal når vagusnerven kan den initiera en serie neurofysiologiska svar:
- Neurotransmitter-modulering: Stimulering kan utlösa acetylkolinfrisättning vid parasympatiska terminaler, vilket stöder en övergång från sympatisk dominans mot parasympatisk aktivitet och aktiverar antiinflammatoriska vägar
- Brainstem nucleus aktivering: Afferenta vagala signaler projicerar till nucleus tractus solitarius, som integrerar autonom regleringsinformation och påverkar tarm-hjärnkommunikationscentra i medulla
- Autonom rebalansering: Konsekvent stimulering kan stödja en gradvis förskjutning i autonom balans, förbättra HRV och potentiellt minska visceral överkänslighet över tid
- Neuroplastisk anpassning: Hållbara VNS-protokoll kan stödja omorganisation av centrala autonoma nätverk, en viktig övervägning med tanke på att förändringarna är gradvis snarare än omedelbar
- Inflammatorisk modulering: Vagal stimulation activates the cholinergic anti-inflammatory pathway, which may help reduce the low-grade inflammatory signalling associated with gut barrier dysfunction and mucosal reactivity in some IBS presentations
Vetenskapliga Parametrar
Forskningsprotokoll för vagal neuromodulering använder vanligtvis:
- Sessionens varaktighet: De flesta protokoll rekommenderar 30 – 60 minuters daglig användning för optimala resultat, men kortare 15-minuters sessioner kan fortfarande ge fördelar för vissa individer.
- Intensitet: Kalibrerad till individuell sensorisk tröskel; märkbar men bekväm, utan smärta
- Konsekvens: Daglig applicering under minst 8 – 12 veckor, eftersom de neuroplastiska och autonoma förändringarna i samband med denna strategi kräver långvarig, konsekvent användning
Förväntad Tidslinje
VNS stöder gradvis anpassning av nervsystemet snarare än omedelbart symptomundertryckning. Baserat på tillgänglig forskning:
Vecka 1 – 2: Många märker en mild förändring i deras allmänna stressrespons under och efter sessioner, och vissa rapporterar blygsamma sömnförbättringar. Förändringar i matsmältningssymtom är vanligtvis begränsade i detta skede.
Vecka 3 – 4: Vissa människor börjar märka förändringar i tarmreaktivitet: måltiderna känner sig mindre belastade, uppblåst och kramper episoder minskar i intensitet eller frekvens, tarmmmönstren blir något mer konsekvent.
Månad 2 – 3: För människor som svarar tenderar mer meningsfulla förändringar att dyka upp under denna period: större tarmregularitet, minskad visceral känslighet, förbättrad HRV, minskat beroende av symptomhanteringsstrategier och en växande förmåga att tolerera tidigare undvikna livsmedel.
Månad 3+: För dem som fortsätter, ytterligare stabilisering av tarm-hjärnreglering, minskning av tarmrelaterade oroliga tankar och kognitiv belastning och förbättrad funktionell kapacitet inklusive större flexibilitet kring mat, resor och planering.
Enskilda svar varierar avsevärt, och dessa tidsramar är inte en garanti för specifika resultat. Denna strategi används bäst som en del av en bredare, betraktad tarm-hjärnstödstrategi snarare än som en fristående lösning.
Säkerhetsöverväganden
Transkutan aurikulär vagusnervstimulering har en generellt gynnsam säkerhetsprofil i publicerad forskning. Potentiella övergående svar kan inkludera:
- Mild stickande känsla på stimuleringsplatsen på örat
- I fall av tillfällig lokal irritation kan vissa protokoll växla öron för att minska upprepad kontakt på samma stimuleringsplats, beroende på enhetens vägledning.
Viktig: Detta tillvägagångssätt är inte lämpligt för individer med hjärtpacemakare eller implanterade elektriska apparater, under graviditet eller hos personer med en historia av vagotomi. Enskilda omständigheter är viktiga.
Om du har en komplex sjukhistoria eller för närvarande tar medicin som påverkar det autonoma nervsystemet är det värt att granska enhetens vägledning och prata med din vårdgivare innan du börjar.
Persistenta tarmsymtom kopplade till vagusnervdysfunktion och dysreglering av tarm-hjärnaxlar är ett område med äkta och växande vetenskapligt intresse.
Forskningen om icke-invasiv vagal neuromodulering utvecklas fortfarande, men det är tillräckligt materiellt för att göra detta till en rimlig strategi att utforska för utvalda individer, tillsammans med snarare än istället för andra strategier.
Informationen på denna sida tillhandahålls för utbildningsändamål och utgör inte specifik medicinsk rådgivning eller ersättning för professionell diagnos eller behandling. VNS-enheter är inte avsedda att diagnostisera, behandla, bota eller förebygga någon sjukdom. Individer med IBS eller ihållande tarmsymtom bör samarbeta med kvalificerade vårdgivare för att utveckla omfattande, personliga förvaltningsstrategier. Kontakta alltid din läkare innan du påbörjar någon ny intervention, särskilt om du har en komplex sjukhistoria eller tar medicin. Rekommenderas av Star Freudenberg och Star Freud Wellness Clinic som ett tilläggssätt för utvalda patienter där dysreglering av tarm-hjärnaxlar verkar vara en kliniskt relevant del av bilden. Individuella resultat kan variera.
Källorv
- Bonaz B, Sinniger V, Pellissier S. Vagus nerve stimulation at the interface of brain-gut interactions. Cold Spring Harb Perspect Med. 2019;9(8):a034199.
- Bonaz B, Bazin T, Pellissier S. The vagus nerve at the interface of the microbiota-gut-brain axis. Front Neurosci. 2018;12:49.
- Farmer AD, Aziz Q. Visceral pain hypersensitivity in functional gastrointestinal disorders. Br Med Bull. 2009;91(1):123-136.
- Sowder E, Gevirtz R, Shapiro W, Ebert C. Restoration of vagal tone: a possible mechanism for functional abdominal pain. Appl Psychophysiol Biofeedback. 2010;35(3):199-206.
- Pellissier S, Dantzer C, Canini F, Mathieu N, Bonaz B. Psychological adjustment and autonomic disturbances in inflammatory bowel diseases and irritable bowel syndrome. Psychoneuroendocrinology. 2010;35(5):653-662.
- Mayer EA, Naliboff BD, Craig AD. Neuroimaging of the brain-gut axis: from basic understanding to treatment of functional GI disorders. Gastroenterology. 2006;131(6):1925-1942.
- Breit S, Kupferberg A, Rogler G, Hasler G. Vagus nerve as modulator of the brain-gut axis in psychiatric and inflammatory disorders. Front Psychiatry. 2018;9:44.
- Kovacic K, Hainsworth K, Sood M, et al. Neurostimulation for abdominal pain-related functional gastrointestinal disorders in adolescents: a randomised, double-blind, sham-controlled trial. Lancet Gastroenterol Hepatol. 2017;2(10):727-737.
Dela via:

